
Primary brain cancer refers to malignant tumors that form either in the brain or in the nerves originating in the brain.1 Brain cancer does not frequently spread (metastasize) to outside of the central nervous system (CNS). The CNS is the part of the nervous system that includes the brain and spinal cord.2, 3, 4Primary brain cancer makes up 2% to 3% of all new cancer cases in adults and is the second most common form of childhood cancer (after leukemia). Brain cancer is the leading cause of cancer deaths in children aged 1-19 years and primary brain cancers caused 40% of cancer deaths in adults from 2012-2016.5, 6
Secondary brain cancer refers to malignant tumors that originated elsewhere but have spread (metastasized) to the brain. Examples include, but are not limited to, breast cancer and lung cancer that have metastasized to the brain. Secondary brain cancer is more common than primary brain cancer.7, 1.
Brain cancer rates are found to be higher in more developed countries than in less developed countries.8The American Cancer Society estimates that in 2023, in the U.S., about 24,810 individuals will be diagnosed with brain or spine cancer and about 18,990 individuals will die of brain or spinal cord tumors.9
Please visit the following sections to learn more about brain cancer:
- Brain anatomy and function
- Brain cancer types
- Brain cancer risks factors
- Brain cancer symptoms and detection
- Brain cancer staging and pathology
- Brain cancer tumor biology
- Brain cancer treatments
- Brain cancer resources
- Section Summary: Brain Cancer
Brain Anatomy And Function
The brain and the spinal cord make up the central nervous system (CNS). The brain, an extremely complex organ, contains more than a trillion neurons. These neurons work together to give us the ability to understand, comprehend, reason, and remember. Since many regions of the brain intricately work together to accomplish certain tasks, it may be difficult to pinpoint a specific region that is solely responsible for a certain brain activity.
The 3 main parts of the brain are the forebrain, the cerebellum, and the brain stem. The forebrain includes the cerebrum and the diencephalon. The cerebrum is seperated into a left and a right hemisphere and is the most frontal part of the brain. The diencephalon includes parts of the brain such as the thalamus and hypothalamus, which are responsible for controling, emotion, pain, body temperature, and stress. More information on these parts are found below. The brain and spinal cord are protected by several layers of connective membrane tissue, collectively known as the meninges.10, 11The CNS is also protected by cerebrospinal fluid (CSF), a colorless fluid that is secreted by four hollow structures of the brain known as ventricles. The CSF helps absorb shocks or blows to the head and is responsible for regulating and maintaining the proper chemical environment necessary for optimal CNS function. 12

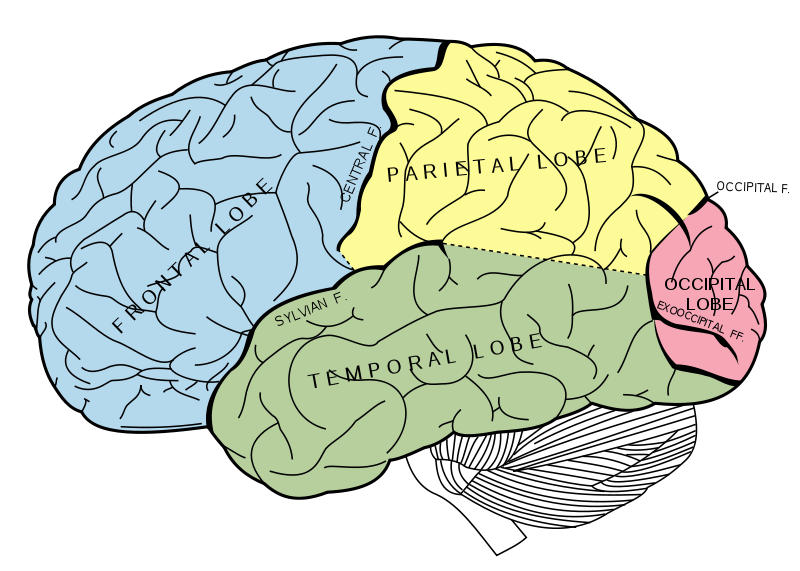
Principal fissures and lobes of the cerebrum viewed laterally. Figure 728 from Gray's Anatomy.13
Some functions of the brain regions:
- Forebrain: The forebrain consists of the cerebrum and the diencephalon. This region is responsible for perception, learning, memory, skeletal-muscle coordination, awareness, regulation of behaviors (e.g. eating and drinking), control of body temperature, and the generation of emotions.
- Cerebellum: The cerebellum is responsible for the coordination of movement and the control of posture and balance.12
- Brain stem: The brain stem consists of the midbrain, pons, and medulla oblongata.12The brainstem relays information between the spinal cord, forebrain, and cerebellum, and it has several important functions of its own. The brainstem controls movement, breathing, heart functions, and the regulation of sleep/conciousness.10, 11
Cells of the brain:
Like all other organs, the brain is also composed of many different types of cells. The cells that are most prevalent to brain cancer are:
- Nerve cells (neurons): Nerve cells are responsible for transmitting signals from the brain to the spinal cord and the body, and these cells are also responsible for bringing signals from the rest of the body back to the brain.
- Glial cells: Glial cells support neurons by insulating them, feeding them, and providing them with structural support. These cells are also responsible for getting rid of dead neurons. There are several different types of glial cells, each with its own function. Glial cell types include astrocytes, oligodendrocytes, and ependymal cells.
Types
There are over 100 types of cancer that can affect the central nervous system (CNS).14 As mentioned previously, cancers that arise in other locations (breast, lung, etc.) and spread (metastasize) to the brain are not considered brain cancer. They are still treated as the cancers of the original site. Here, we will only discuss primary brain cancers (those that originate in the brain).
Gliomas
Malignant gliomas are the most common and deadly brain cancers. They originate in the glial cells of the central nervous system (CNS). Gliomas can be divided into 3 main types: astrocytomas, oligodendrogliomas, and ependymomas.15 The median survival of patients with glioma has improved over the past few years but is still only 15 months, with few patients living more than two years.16 Research indicates that this type of brain cancer may resist treatment because it contains stem cells that are responsible for driving the formation of blood vessels (angiogenesis), spread of the tumor (metastasis), and resistance to treatments.17, 18
- Astrocytomas: Astrocytomas are tumors that develop in astrocytes and are found in the cerebrum and the cerebellum. Astrocytomas make up approximately 50% of all primary brain tumors. Glioblastoma multiforme, an astryocytoma subtype, is the most aggressive form of brain cancer and is associated with poor prognosis.19
- Oligodendrogliomas: Oligodendrogliomas are tumors that develop in oligodendrocytes, and more often in the oligodendrocytes that are found in the cerebral hemispheres. Oligodendrocytes are glial cells that produce myelin, a component of the brain that increases impulse speed. 20Oligodendrogliomas make up approximately 4% of primary brain tumors. Approximately 55% of all cases of oligodendrogliomas appear in people between the ages of 40 and 64.21, 19
- Ependymomas: Ependymomas are tumors that develop in the ependymal cells. Ependymal cells are the cells in the brain and where ceribrospinal fluid (CSF) is created and stored. 22Ependymomas account for only 2% to 3% of all primary brain tumors but account for 8% to 10% of brain tumors in children. Ependymoma tumors are usually found in ventricle linings, the spinal cord, or the regions near the cerebellum.19
Nongliomas
Nongliomas are tumors that do not arise from glial cells. More prevalent examples of nongliomas include meningiomas and medulloblastomas. Less prevalent examples include medullpituitary adenomas, primary CNS lymphomas, and CNS germ cell tumors.
- Meningiomas: Meningiomas are tumors that develop in the meninges, membranes covering the brain and spinal cord. Meningioma tumors are frequently formed from arachnoid cells. These cells are responsible for the absorption of the cerebrospinal fluid (CSF). Meningioma tumors are responsible for 13% to 30% of all tumors arising within the cranium - the bony case surrounding the brain. Tumor arising within the cranium are also called intracranial tumors. Most meningiomas are benign. Malignant meningiomas are extremely rare, with an incidence rate of approximately two out of every million people, per year. The risk for developing meningiomas increases with age and is more prevalent in women.23, 24
- Medulloblastomas: Medulloblastomas are the most common brain malignancies in children. These cancers arise in the posterior fossa - a specific region of the space inside the skull (intracranial cavity) that contains the brainstem and the cerebellum. The fourth ventricle region is involved in the development of approximately 80% of childhood cases.25, 26
Risks
For most types of brain cancer, specific risk factors have not yet been identified. However, some risk factors (and potential risk factors) have been described. They include:
1. Age: The risk of most cancers increases with age. However, neuroblastoma is an exception; it most commonly occurs in young children.
2. Heredity: Some genetic disorders have been identified as possible risk factors for brain cancer. They include:
a. Neurofibromatosis type 1: A condition characterized by changes in skin color and the growth of small tumors on the skin, brain and other parts of the body. People with this condition have a greater risk of developing shwannomas, meningiomas, neurofibromas, and other types of gliomas. Adults with this condition develop cancerous tumors that grow along the nerves.27
b. Neurofibromatosis type 2: This is a less common condition than Neurofibromatosis type 1. Mutations in the NF2 gene are linked to this disease. In approximately 50% of all neurofibromatosis type 2 cases, the NF2 gene mutation is inherited from the parents.This disease may be associated with acoustic neuromas, meingiomas, and spinal cord ependymomas. The signs and symptoms of this condition usually appear during adolescence or when individuals reach their early twenties (18-24 years old). Some symptoms include balance dysfunction and hearing loss. 28
c. Tuberous sclerosis: This is an inherited genetic disorder that causes tumor growths in the skin, brain/nervous system, kidneys, and heart. The tumors of this disease tend to be non-cancerous tumors (benign), but may become cancerous. Most cases of tuberous sclerosis are due to random mutations in the TSC1 and TSC2 genes. There are no known risk factors for this disease apart from having a parent with the disease. In most cases, however, there are usually no familial history of tuberous sclerosis.29
d. Von Hippel-Lindau (VHL) syndrome: This condition is associated with the development of benign and malignant tumors in different parts of the body. The VHL gene is a tumor suppressor gene that is responsible for this syndrome. Mutations in the VHL gene produce abnormal VHL proteins that cannot properly regulate cell survival and cell proliferation.30
e. Li-Fraumeni syndrome: This rare condition is associated with a greater risk of developing gliomas and other types of cancer. Studies show that the CHEK2 gene and the TP53 gene are linked to Li-Fraumeni syndrome. About half of the families with Li-Fraumeni syndrome have inherited mutations in the TP53 gene.31
3. Infections: Viruses, such as retroviruses, papovaviruses and adenoviruses, have been shown to cause brain tumors in animals, but few studies show links between viral infections and brain cancer in humans. However, viruses have not yet been dismissed as a possible risk factor and research is still ongoing in this area.32
4. Head injury and trauma: The possible relationship between head injuries and meningiomas is currently being studied. Studies have found that many children diagnosed with brain tumors had head injuries/head trauma during birth.32
5. Vitamins: Studies suggest a possible link between the consumption of N-nitroso compounds during pregnancy and an increased risk of brain tumor development in offsprings.32, 33, 34
Get information about brain cancer treatments from the Winship Cancer Institute of Emory University.
Symptoms And Detection
Brain tumor symptoms depend on the tumor's size, location, type and if/how much the tumor has invaded other areas of the body. The most common symptom is headaches, which occurs in 35% of patients and can appear along with nausea, vomiting, and problems with a variety of specific nerve functions, called focal neurological deficits. Headaches may be a warning sign, especially in patients who normally do not suffer from headaches. Localized (focal) problems vary depending on the tumor’s location. It is also important to inform the patient's doctor if headaches become increasingly frequent or severe.35
Several medical tests can be used to detect or rule out a brain tumor:
- Neurological exam: The neurological exam refers to a preliminary set of tests performed on a patient in order to gather information on his/her mental state, sensory system, nervous system, and motor functions. Based on the neurological exam results, the physician will then decide if additional tests are necessary.36Learn more about neurological exams.
Cerebral angiography: A cerebral angiography is a procedure performed on a patient to visualize the blood flow through the blood vessels in the patient’s brain. This procedure is done to identify possible blood clots and blood vessel problems in the brain, such as aneurysms, arterial blockages, and vasculitis. This procedure may also be used to confirm the presence of a brain tumor.
How it works
Cerebral angiography is typically done in the hospital or in a radiology center. The patient may be told not to consume solid foods or liquids for a certain period of time leading up to the test. For the procedure, the patient will be lying on an x-ray table with his/her head immobilized by a strap, tape, etc. This is to prevent any possible movement that may disrupt the exam. An electrocardiogram (ECG) will be used to monitor the patient’s heart activity during the cerebral angiography. Right before the start of the procedure, a local numbing shot (anesthetic) will be administered in the region of the patient's body (usually the groin) where a thin tube (catheter) will subsequently be inserted. The catheter will go into an artery and will be carefully manuevered upwards, through the abdominal area, towards an artery in the patient's neck. Once the catheter is in its intended position, a special dye will be injected into it, and x-ray scans will be taken as a method of tracking the dye’s movement through the arteries and blood vessels in the brain. These x-ray scans will allow the doctor to identify the location of any arterial and vascular blockages and locate any possible abnormal vascular and arterial structural defects in the patient’s brain.37
- CT scan: Learn more about CT scans.
- MRI scan: Learn more about MRI scans.
- Surgical biopsy: Learn more about biopsies.
Staging And Pathology
If there is suspicion that a person may have brain cancer, a sample of tissue (biopsy) may be taken for examination. After a surgical biopsy is taken, the physician who performed it sends the specimen to a neuropathologist. A neuropathologist is a pathologist who specializes in nervous system disorders. The neuropathologist examines the specimen at both the macroscopic (visible with the naked eye) and microscopic (requiring magnification) levels and provides a pathology report to the physician. The pathology report contains information about the tissue's appearance, cellular make-up, and state of disease or normalcy. For more information about pathology reports, refer to the Diagnosis & Detection section.
For an accurate pathology report, it is extremely important that it be made by an expert in neourpathology.35
According to the American Cancer Society, due to the many factors that are involved in central nervous system (CNS) cancers, brain cancer does not have a specific staging system that is capable of accurately predicting the cancer's development and likely outcome. The T/N/M staging system is not an appropriate tool either because most brain and spine cancers are unable to spread to other organs (metastasize).38The World Health Organization (WHO), however, has developed a histological classification system that focuses on the tumor's biological behavior. This system can be used to classify central nervous system cancers by grading (I to IV) the tumors based on the their characteristics. Once this grading information is analyzed along with the other available clinical data, a prognosis can then be made. Grade I to II tumors (lower grade tumors) have some abnormal structures, but these tumors look like normal brain tissues, for the most part. Grade III tumors have more abnormal features, increased numbers of blood vessels, and higher cell densities. Grade IV tumors are the most malignant primary brain tumors. The cancerous cells of Grade IV tumors have the most abnormal features. These tumors have increased numbers of blood vessels, increased cell growth, and very high cell densities.39
Tumor Biology
In recent years, studies have suggested that cancer stem cells, or more specifically, glioma stem cells, may have an important role in brain cancer development and tumor relapse. CD133 is a protein found on the surface of cells. It is a stem cell marker that is commonly used to identify brain tumor stem cells (BTSCs). BTSCs have been found in types of brain cancer such as glioblastoma multiforme, ependymomas, astrocytomas, medulloblastomas, and other glioma and nongliomas. BTSCs may be resistant to treatment with chemotherapy and/or radiation due to a variety of factors, including the overexpression of anti-cell death (antiapoptotic) factors, activation of DNA repair checkpoints, and increased blood vessel development (angiogenesis).40
There are many genes that have been linked to the development and spread of brain cancer, with some more prevalent than others. Some of the genes involved in brain cancer are:
- TP53: This gene is a tumor suppressor gene that is in charge of regulating cell division and cell death (apoptosis). About half of all human tumors have a mutation in the TP53 tumor suppressor gene. Studies have shown that approximately 40% of astrocytomas have a mutated or deleted TP53 gene.32
- NF1: This gene encodes for the production of neurofibromin. The neurofibromin protein acts as a tumor suppressor by regulating the expression of Ras, another protein involved in cancer development.41
- NF2: This gene encodes for the merlin protein, which regulates cell shape, cell movement, and cell-to-cell communication. The merlin protein also acts as a tumor suppressor in the cells of the nervous system. Studies show that the NF2 gene is deleted or mutated in approximately 40% to 50% of patients with meningioma or schwannoma.42, 32
- Bcl2: This gene encodes for the Bcl2 protein, which inhibits cell death. Studies suggest that overexpression of the Bcl2 protein significantly increases tumor resistance to cytotoxic drugs.43
- Myc: This family of genes encodes for the Myc transcription factor proteins, which are involved in tumorigenesis and cell cycle regulation. The Myc proteins are overexpressed in many types of gliomas, including medulloblastoma, astrocytomas, and glioblastoma multiforme.44, 45
- EGFR: This gene encodes for the epidermal growth factor receptor (EGFR).46 EGFR belongs to the family of receptor tyrosine kinases (RTK), which are cell surface receptors that bind to cell signaling factors such as growth factors and cytokines. Increased RTK signaling through two oncogenic pathways called the PI3K-AKT-mTOR pathway and the Ras-MAPK pathway have been linked to cases of malignant gliomas.47 Studies show that approximately 40% of gioblastomas and anaplastic astrocytomas have too many copies of the EGFR gene (gene amplification) and/or changes (mutations) in the EGFR gene.32, 48
- VEGF: This gene encodes for the vascular endothelial growth factor (VEGF), which is a key protein involved in blood vessel formation (angiogenesis) and vascular permeability. Its receptor, vascular endothelial growth factor receptor (VEGFR), also belongs to the family of receptor tyrosine kinases (RTK). Studies show that VEGF is commonly overexpressed in meningiomas, as well as in malignant gliomas, such as pilocytic astrocytomas and glioblastomas.49
Treatment
Treatment options for brain cancer depend on the tumor's location, the degree to which the tumor is affecting brain and spinal cord functions, and the patient’s health history. Some treatment options include chemotherapy, radiation therapy, surgery and ancillary therapeutic agents.35
Since Cancer Quest's focus is on the cancer's biology and the biology of possible treatments, we do not give detailed treatment guidelines. Instead, we link to organizations in the U.S. that do generate treatment guidelines.
For more information about how the above-mentioned cancer treatments work, refer to the Cancer Treatments section.
Information about clinical trials:
General clinical trial information from CancerQuest
Click here for information about clinical trials from the National Cancer Institute.
Click here for information about clinical trials from Georgia Clinical Trials Online.
Brain Cancer Resources
Risks for Brain Cancer
Brain Tumor Risk Factors (ABTA)
Risk Factors for Brain and Spinal Cord Tumors (ACS)
Brain Cancer Risk Factors (CTCA)
Detection and Diagnosis of Brain Cancer
Winship Cancer Insitute: Brain Tumor Diagnosis & Staging
Brain and Spinal Tumors in Adults (ACS)
Brain and Spinal Tumors in Children (ACS)
Brain Cancer Treatments
Brain Tumor Trials and Treatment
Adult Central Nervous System Tumors Treatment (NCI)
Childhood Brain and Spinal Cord Tumors Treatment (NCI)
Brain Cancer Treatment Options
Brain Cancer Survivorship
Childhood Brain Tumor Foundation
Long Term Risks for Brain Cancer Survivors
Possible Side Effects of Radiation Treatment for Brain Tumors (OncoLink)
Side Effects From Radiation Therapy to the Brain
International Resources
Brain Tumor Foundation of Canada
Dharamshila Hospital Brain Cancer Information (India)
Brain Tumors and Treatment in India (Mediconnect)
Cancer Council Australia: Brain Cancer
Brain Tumours (Cancer Research UK)
Section Summary
Introduction
- Primary brain cancer is the leading cause of cancer deaths in children.
- Primary brain cancer is the third most common cause of cancer deaths in adults aged 15 to 34.
Types of Brain Cancer
- Primary brain cancer can be categorized into 2 types: gliomas and nongliomas.
- Malignant gliomas originate in the glial cells of the CNS and are the more common and more lethal form of brain malignancies. There are 3 main types of gliomas: astrocytomas, oligodendrogliomas, and ependymomas.
- Nongliomas do not originate in the glial cells of the CNS. These tumors develop in other parts of the brain. Some examples of nongliomas include meningiomas and medulloblastomas.
Risk Factors
- Genetic disorders, such as neurofibromatosis type 1 and type 2, have been identified as possible risk factors for brain cancer.
- Brain cancer risk increases with age, with the exception of neuroblastoma, which commonly occurs in young children.
- The possible relationship between head injuries and meningiomas is still under investigation.
- Consumption of N-nitroso compounds during pregnancy may be linked to an increased risk of brain tumor development in offsprings.
Symptoms and Detection
- Headaches may be a warning sign of brain tumors.
- Several medical tests can be used to detect or rule out a brain tumor. Examples include: neurological exams, cerebral angiographies, CT scans, MRI scans, and surgical biopsies.
Staging and Pathology
- Brain cancer does not have a specific staging system that is capable of accurately predicting the cancer's development and likely outcome. The T/N/M system is not an appropriate tool for brain cancer because most brain and spine cancers are unable to spread to other organs (metastasize).
- Brain cancer is classified based on the World Health Organization's (WHO) histological classification system, which focuses on the tumor's biological behavior.
Treatment
- Treatments differ depending on specific factors, such as the patient's age, patient's health conditions, cancer stage, tumor's location, and more.
- Treatments can include surgery, radiation therapy, chemotherapy, resection, and ancillary therapeutic agents.
- 1ab Lu-Emerson C, Eichler AF. Brain metastases. Continuum (Minneap Minn). 2012 Apr;18(2):295-311. [PUBMED]
- 2 Volavsek M, Lamovec J, Popovic M. Extraneural metastases of anaplastic oligodendroglial tumors. Pathol Res Pract. 2009;205(7):502-7. Epub 2009 May 2. [PUBMED]
- 3 Kural C, Pusat S, Sentürk T, Seçer HI, Izci Y. Extracranial metastases of anaplastic oligodendroglioma. J Clin Neurosci. 2011 Jan;18(1):136-8. [PUBMED]
- 4 Dafny N, Neuroscience Online “Chapter 1: Overview of the Nervous System”, Department of Neurobiology and Anatomy, The UT Medical School at Houston. Copyright 1997-2020. (Accessed Feb. 21, 2020) [ http://nba.uth.tmc.edu/neuroscience/s2/chapter01.html]
- 5 American Cancer Society. Cancer Facts & Figures 2019. Atlanta: American Cancer Society; 2019. (Accessed Feb. 21, 2020) [ https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2019/cancer-facts-and-figures-2019.pdf]
- 6 Curtin SC, Miniño AM, Anderson RN.Declines in Cancer Death Rates Among Children and Adolescents in the United States, 1999–2014, NCHS Data Brief, September 2016, No. 257. (Accessed February 21, 2020) [https://www.cdc.gov/nchs/data/databriefs/db257.pdf]
- 7 Nguyen TD, Abrey LE. Brain metastases: old problem, new strategies. Hematol Oncol Clin North Am. 2007;21(2):369-388. [PUBMED]
- 8 Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005 Mar-Apr;55(2):74-108. [PUBMED]
- 9 American Cancer Society. Cancer Facts & Figures 2023. Atlanta: American Cancer Society; 2023. https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/2023-cancer-facts-figures.html]
- 10ab Human Physiology: The Mechanisms of Body Function. AJ Vander, J Sherman, D Luciano, EP Widmaier, H Raff, H Strang; published by McGraw-Hill, New York (2004).
- 11ab Neuroscience. 2nd edition. Purves D, Augustine GJ, Fitzpatrick D, et al., editors. Sunderland (MA): Sinauer Associates; 2001. [http://www.ncbi.nlm.nih.gov/books/NBK10799/]
- 12abc Brain Components. Medline Plus. [http://www.nlm.nih.gov/medlineplus/ency/anatomyvideos/000016.htm]
- 13 Brain Lobe image. Wikipedia [http://www.cancerquest.org/sites/default/files/assets/image/brain-lobes.png]
- 14 Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, Scheithauer BW, Kleihues P. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007 Aug;114(2):97-109. Epub 2007 Jul 6. [PUBMED]
- 15 Parsons DW, Jones S, Zhang X, Lin JC, Leary RJ, Angenendt P, Mankoo P, Carter H, Siu IM, Gallia GL, Olivi A, McLendon R, Rasheed BA, Keir S, Nikolskaya T, Nikolsky Y, Busam DA, Tekleab H, Diaz LA Jr, Hartigan J, Smith DR, Strausberg RL, Marie SK, Shinjo SM, Yan H, Riggins GJ, Bigner DD, Karchin R, Papadopoulos N, Parmigiani G, Vogelstein B, Velculescu VE, Kinzler KW. An Integrated Genomic Analysis of Human Glioblastoma Multiforme. Science. 2008 Sep 26;321(5897):1807-12. doi: 10.1126/science.1164382. Epub 2008 Sep 4. [PUBMED]
- 16 Van Meir EG, Hadjipanayis CG, Norden AD, Shu HK, Wen PY, Olson JJ. Exciting new advances in neuro-oncology: the avenue to a cure for malignant glioma. CA Cancer J Clin. 2010 May-Jun;60(3):166-93. [PUBMED]
- 17 Huang Z, Cheng L, Guryanova OA, Wu Q, Bao S. Cancer stem cells in glioblastoma--molecular signaling and therapeutic targeting. Protein Cell. 2010 Jul;1(7):638-55. Epub 2010 Jul 29. [PUBMED]
- 18 Frosina G. Frontiers in targeting glioma stem cells. Eur J Cancer. 2011 Mar;47(4):496-507. Epub 2010 Dec 22. [PUBMED]
- 19abc Mesfin, F. B., & Al-Dhahir, M. A. (2020). Cancer, Brain Gliomas. Treasure Island (FL): StatPearls Publishing. (Original work published January 2020) [PUBMED]
- 20 Dugdale, D. C. (2013, April 18). Myelin. [http://www.nlm.nih.gov/medlineplus/ency/article/002261.htm]
- 21 Van den Bent MJ, Reni M, Gatta G, Vecht C. Oligodendroglioma. Crit Rev Oncol Hematol. 2008 Jun;66(3):262-72. Epub 2008 Feb 12. [PUBMED]
- 22 National Brain Tumor Society. Tumor types- ependymomas. [http://braintumor.org/brain-tumor-information/understanding-brain-tumors/tumor-types/#Ependymoma]
- 23 Marta GN, Correa SF, Teixeira MJ. Meningioma: review of the literature with emphasis on the approach to radiotherapy. Expert Rev Anticancer Ther. 2011 Nov;11(11):1749-58. [PUBMED]
- 24 Link M., and Perry, A. Meningioma Tumorigenesis: An Overview of Etiologic Factors. From 'Meningiomas'. Published by Springer London. Joung Lee, Editor (2009) [http://dx.doi.org/10.1007/978-1-84628-784-8_11]
- 25 Schroeder K, Gururangan S. "Molecular variants and mutations in medulloblastoma." Pharmgenomics Pers Med. 2014 Feb 4;7:43-51. eCollection 2014. [PUBMED]
- 26 General Information About Central Nervous System (CNS) Embryonal Tumors. Childhood Central Nervous System Embryonal Tumors Treatment (PDQ®) [http://www.cancer.gov/cancertopics/pdq/treatment/childCNSembryonal/healthprofessional#Section_633]
- 27 Williams VC, Lucas J, Babcock MA, Gutmann DH, Korf B, Maria BL. Neurofibromatosis type 1 revisited. Pediatrics. 2009 Jan;123(1):124-33. doi: 10.1542/peds.2007-3204. [PUBMED]
- 28 Evans GR, Lloyd SK, Ramsden RT. Neurofibromatosis type 2. Adv Otorhinolaryngol. 2011;70:91-8. doi: 10.1159/000322482. Epub 2011 Feb 24. [PUBMED]
- 29 Wu J, Shin J, Xie D, Wang H, Gao J, Zhong XP. Tuberous Sclerosis 1 Promotes Invariant NKT Cell Anergy and Inhibits Invariant NKT Cell-Mediated Antitumor Immunity. J Immunol. 2014 Feb 14. [PUBMED]
- 30 Sharma P, Dhull VS, Bal C, Malhotra A, Kumar R. Von Hippel-Lindau Syndrome: Demonstration of Entire Disease Spectrum with (68)Ga-DOTANOC PET-CT. Korean J Radiol. 2014 Jan;15(1):169-72. doi: 10.3348/kjr.2014.15.1.169. Epub 2014 Jan 8. [PUBMED]
- 31 Malkin D. Li-fraumeni syndrome. Genes Cancer. 2011 Apr;2(4):475-84. doi: 10.1177/1947601911413466. [PUBMED]
- 32abcdef Wrensch M, Minn Y, Chew T, Bondy M, Berger MS. Epidemiology of primary brain tumors: current concepts and review of the literature. Neuro Oncol. 2002 Oct;4(4):278-99. [PUBMED]
- 33 McKean-Cowdin R, Pogoda JM, Lijinsky W, Holly EA, Mueller BA, Preston-Martin S. Maternal prenatal exposure to nitrosatable drugs and childhood brain tumours. Int J Epidemiol. 2003 Apr;32(2):211-7. [PUBMED]
- 34 Huncharek M, Kupelnick B. "A meta-analysis of maternal cured meat consumption during pregnancy and the risk of childhood brain tumors." Neuroepidemiology (2004); 23(1-2):78-84. [PUBMED]
- 35abc Buckner JC, Brown PD, O'Neill BP, Meyer FB, Wetmore CJ, Uhm JH. Central nervous system tumors. Mayo Clin Proc. 2007 Oct;82(10):1271-86. Review. [PUBMED]
- 36 Fritz, D., & Musial, M. (2016). Neurological Assessment. Home Healthcare Now, 34(1), 16–22. http://doi.org/10.1097/NHH.0000000000000331 (Original work published January 2016) [PUBMED]
- 37 Cerebral Angiography. MedlinePlus. [http://www.nlm.nih.gov/medlineplus/ency/article/003799.htm]
- 38 "How are brain and spinal cord tumors in adults staged?" American Cancer Society. [http://www.cancer.org/Cancer/BrainCNSTumorsinAdults/DetailedGuide/brain-and-spinal-cord-tumors-in-adults-staging]
- 39 Persano L, Rampazzo E, Basso G, Viola G. "Glioblastoma cancer stem cells: role of the microenvironment and therapeutic targeting." Biochem Pharmacol. 2013 Mar 1;85(5):612-22. doi: 10.1016/j.bcp.2012.10.001. Epub 2012 Oct 11. [PUBMED]
- 40 Cheng JX, Liu BL, Zhang X. "How powerful is CD133 as a cancer stem cell marker in brain tumors?" Cancer Treat Rev. 2009 Aug;35(5):403-8. doi: 10.1016/j.ctrv.2009.03.002. Epub 2009 Apr 14. [PUBMED]
- 41 Friedman JM. Neurofibromatosis 1. GeneReviews [Internet]. [PUBMED]
- 42 Evans DG. Neurofibromatosis 2. GeneReviews [Internet]. [PUBMED]
- 43 Fels C, Schäfer C, Hüppe B, Bahn H, Heidecke V, Kramm CM, Lautenschläger C, Rainov NG. "Bcl-2 expression in higher-grade human glioma: a clinical and experimental study." J Neurooncol. 2000 Jul;48(3):207-16. [PUBMED]
- 44 Faria MH, Khayat AS, Burbano RR, Rabenhorst SH. "c -MYC amplification and expression in astrocytic tumors." Acta Neuropathol. 2008 Jul;116(1):87-95. doi: 10.1007/s00401-008-0368-0. Epub 2008 Mar 28. [PUBMED]
- 45 Swartling FJ. "Myc proteins in brain tumor development and maintenance." Ups J Med Sci. 2012 May;117(2):122-31. doi: 10.3109/03009734.2012.658975. Epub 2012 Feb 21. [PUBMED]
- 46 Lo HW, Hsu SC, Ali-Seyed M, Gunduz M, Xia W, Wei Y, Bartholomeusz G, Shih JY, Hung MC. Nuclear interaction of EGFR and STAT3 in the activation of the iNOS/NO pathway. Cancer Cell. 2005 Jun;7(6):575-89. [PUBMED]
- 47 Huse JT, Holland EC. "Targeting brain cancer: advances in the molecular pathology of malignant glioma and medulloblastoma." Nat Rev Cancer. 2010 May;10(5):319-31. doi: 10.1038/nrc2818. [PUBMED]
- 48 Hatanpaa KJ, Burma S, Zhao D, Habib AA. Epidermal growth factor receptor in glioma: signal transduction, neuropathology, imaging, and radioresistance. Neoplasia. 2010 Sep;12(9):675-84. [PUBMED]
- 49 Stockhammer G, Obwegeser A, Kostron H, Schumacher P, Muigg A, Felber S, Maier H, Slavc I, Gunsilius E, Gastl G. Vascular endothelial growth factor (VEGF) is elevated in brain tumor cysts and correlates with tumor progression. Acta Neuropathol. 2000 Jul;100(1):101-5. [PUBMED]
{kind=link}